HEALTH DATA RISKS: WHAT PROTECTION FOR SIERRA LEONEANS?
BASITA MICHAEL >>>>> CULLED!
Sierra eye Magazine

Why Sierra Leone Must Publish the Full US Health MOU.
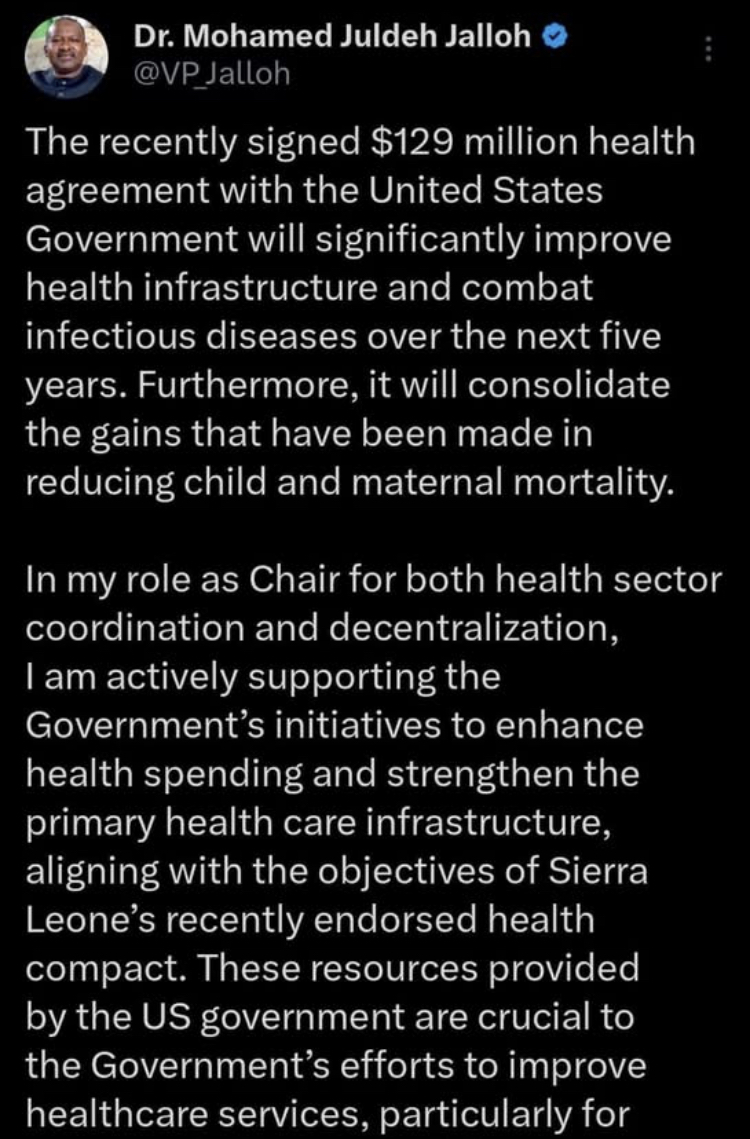
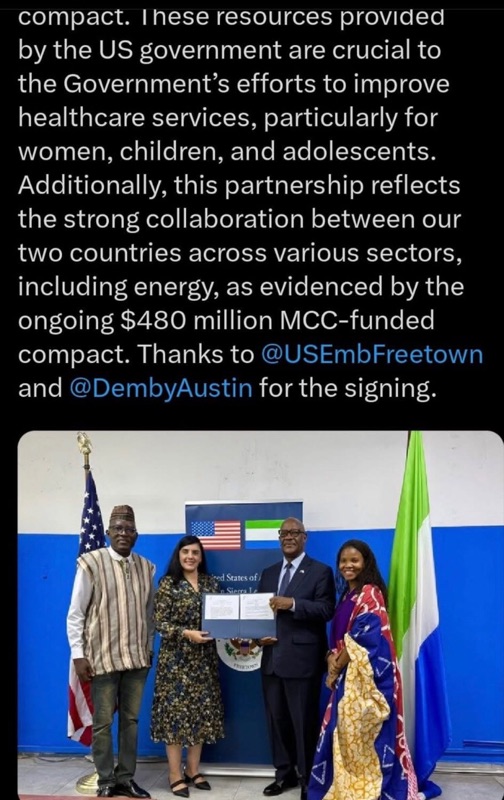
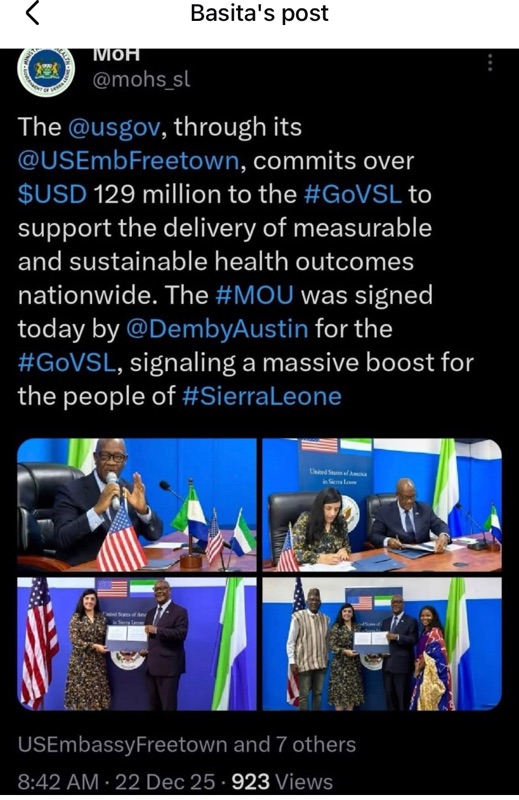
On December 22, 2025, Sierra Leone signed a Memorandum of Understanding (MOU) with the United States on global health cooperation, committing over $129 million in US support over five years. Vice President Dr. Mohamed Juldeh Jalloh hailed it as a boost for health infrastructure, infectious disease control, and reductions in child and maternal mortality. The Ministry of Health on X echoed this, calling it a "massive boost" for measurable and sustainable outcomes.
Yet, days later, the full text of this agreement remains hidden from the public. Sierra Leoneans have seen only celebratory tweets, press releases, and photos of smiling officials holding a closed folder. We are told to trust that this deal serves our interests – but without seeing the document, how can we?
This secrecy is unacceptable. In an era of open governance and accountability, major agreements affecting public health, national budgets, and potentially sensitive citizen data must be transparent. The government owes Sierra Leoneans the right to read, debate, and scrutinise the MOU in full. Publish it now.
This is not a unique bilateral pact. It forms part of the US "America First Global Health Strategy," under which the Trump administration has signed nearly identical five-year MOUs with at least a dozen African countries, including Kenya, Rwanda, Uganda, Liberia, Lesotho, Mozambique, Eswatini, Cameroon, Nigeria, Madagascar, Botswana, and Ethiopia.
These agreements share core elements including front-loaded US funding with a gradual phase-down, the requirements for recipient countries to dramatically increase domestic health spending and assume full responsibility by 2030 for commodities, workforce salaries, and labs, odernisation of electronic medical records, disease surveillance systems, and data infrastructure, sometimes involving US-supported technologies, including satellite-based networking, and measurable performance targets, with potential consequences for non-performance.
For Sierra Leone specifically, it is believed that the US will front-load over $30 million in 2026 to strengthen surveillance, labs, workforce, and data systems. We must by 2030 achieve ambitious goals, including a 75% reduction in malaria deaths, 98% HIV status awareness and treatment, and a national outbreak detection system meeting the international "7-1-7" standard.
These sound positive on paper. But dig deeper, and troubling issues are already sparking legal battles and public outcry elsewhere.
In Kenya, a similar "landmark" $2.5 billion agreement, with the US contributing $1.7 billion, was signed just weeks earlier. Within days, consumer rights groups challenged it in court, alleging risks to personal data privacy and national sovereignty.
On December 11, 2025, Kenya's High Court suspended implementation of the data-sharing provisions pending a full hearing in February 2026. The judge barred any transfer or sharing of "medical, epidemiological, or sensitive personal health data," including potential access to HIV status, TB treatment histories, vaccination records, and more.
Critics argued the deal could expose individual medical records without adequate consent or safeguards, allow US influence over health priorities, and even cede control of digital infrastructure, including cloud storage of raw data, to external entities, potentially benefiting US pharmaceutical companies.
Kenya's government insisted that safeguards exist and that data would be aggregated and de-identified where possible, be governed by Kenyan law, and have no unrestricted access to personal records. Yet the court acted anyway, recognising that promises alone are insufficient without public scrutiny.
Since then, civil society across Africa has warned that these MOUs, negotiated hurriedly and often without parliamentary approval or community input, prioritise US interests in early disease detection and pathogen access over equitable benefit-sharing.
If Sierra Leone's MOU mirrors these others, as US State Department announcements strongly suggest, describing them as standardised bilateral frameworks, it likely includes provisions for real-time or extensive access to national health databases and surveillance systems, sharing of epidemiological data, pathogen samples, and genetic sequencing information and US-supported upgrades to electronic records that could facilitate data flows.
In countries with robust data protection laws, such clauses might be manageable. But Sierra Leone has no comprehensive Data Protection. A Data Protection and Right to Access Information Bill has been in development for years, but it is not yet law. Until then, we have no independent authority to oversee compliance, investigate violations, or penalise misuse.
This vacuum leaves Sierra Leoneans uniquely vulnerable. Sensitive information, such as HIV status in a stigmatised society, maternal health records, and outbreak data from Ebola-scarred communities, could be shared without clear protections. Who ensures de-identification? What prevents third-party access? How do we enforce remedies if breaches occur?
Moreover, these deals are transactional as the funding is tied to performance and data commitments. Failure to meet benchmarks could trigger reductions, disrupting services for women, children, and adolescents, the groups VP Juldeh Jalloh says will benefit most.
While we applaud efforts to secure health funding amid global challenges, such applause must not replace accountability. Release the full MOU text today. Allow parliamentary review, civil society analysis, and public debate. Follow Kenya's lead in addressing concerns head-on and not through tweets, but through transparency. If the deal truly protects sovereignty, privacy, and our health priorities, it has nothing to hide. Secrecy breeds suspicion, openness builds trust.
The health of our nation and the rights of its people demand no less. We deserve a partnership that strengthens us, not one shrouded in shadows.
Austin Demby U.S. Embassy Freetown, Sierra Leone
————————————————
————————————————
https://www.giraffe.org/basita-michael
FURTHER COMMENTS:

th-
Health Minister Signs a Historic $USD 129 Million Health Cooperation Agreement with the U.S. Government..

Freetown, Sierra Leone—Tuesday 23rd Freetown, Sierra Leone—Tuesday 23rd December 2025.
The Government of the Republic of Sierra Leone and the Government of the United States of America have signed a landmark Memorandum of Understanding (MOU) on Health Cooperation, marking a significant milestone in the long-standing partnership to strengthen healthcare and protect populations from the threats of infectious diseases.
This five-year agreement, commencing from 2026 through to 2030, was signed on Monday 22nd December 2025 by the Minister of Health, Dr. Austin Demby, and the Chargé d’Affaires, Rabia M. Qureshi, of the United States Embassy in Freetown.
With this, Sierra Leone becomes one of the first few beneficiary countries in Africa as the U.S Government seeks to explore new ways of doing business with nations around the world.
Signing on behalf of the President, Dr. Julius Maada Bio, Health Minister, Dr. Austin Demby, said;
“This agreement reflects Sierra Leone’s strong leadership and commitment to building a resilient, and self-reliant health system.” Dr. Demby went on; “The MOU is not just about funding—it is about reimagining a new approach to delivering health services by ensuring that partners align their support with our national development aspirations.” 3rd December 2025.
As well as increasing domestic co-investment by Sierra Leone, the funding will deliver measurable and sustainable key health outcomes in four thematic areas including:
· Dramatically reducing deaths from HIV, tuberculosis, malaria, and measles
· Lowering maternal and under-five mortality rates
· Achieving near-universal HIV testing, treatment, and viral suppression
· Strengthening outbreak detection and response within 7 days of emergence
Through this partnership, the Government will prioritize health security, primary health care, and domestic health financing reform, while also protecting data sovereignty, regulatory authority, and national development priorities. A Joint Health Cooperation Steering Committee will oversee implementation, monitor progress, and ensure transparency and accountability.
“With this MOU, we affirm our shared commitment to building resilient, durable health systems, protect people and advance mutually beneficial relationships,” said Rabia M. Qureshi, Chargé d’Affaires of the United States Embassy in Freetown.
The support will also complement Sierra Leone’s progressive greater domestic health financing investment particularly in the areas of recruitmenting frontline health workers, including laboratory staff, and community health workers into the national payroll among other priority areas. d’Af

As well as increasing domestic co-investment by Sierra Leone, the funding will deliver measurable and sustainable key health outcomes in four thematic areas including:
· Dramatically reducing deaths from HIV, tuberculosis, malaria, and measles
· Lowering maternal and under-five mortality rates
· Achieving near-universal HIV testing, treatment, and viral suppression
· Strengthening outbreak detection and response within 7 days of emergence
Through this partnership, the Government will prioritize health security, primary health care, and domestic health financing reform, while also protecting data sovereignty, regulatory authority, and national development priorities. A Joint Health Cooperation Steering Committee will oversee implementation, monitor progress, and ensure transparency and accountability.
“With this MOU, we affirm our shared commitment to building resilient, durable health systems, protect people and advance mutually beneficial relationships,” said Rabia M. Qureshi, Chargé d’Affaires of the United States Embassy in Freetown.
The support will also complement Sierra Leone’s progressive greater domestic health financing investment particularly in the areas of recruitmenting frontline health workers, including laboratory staff, and community health workers into the national payroll among other priority areas.



Comments